Management of USI – Where are we Now?
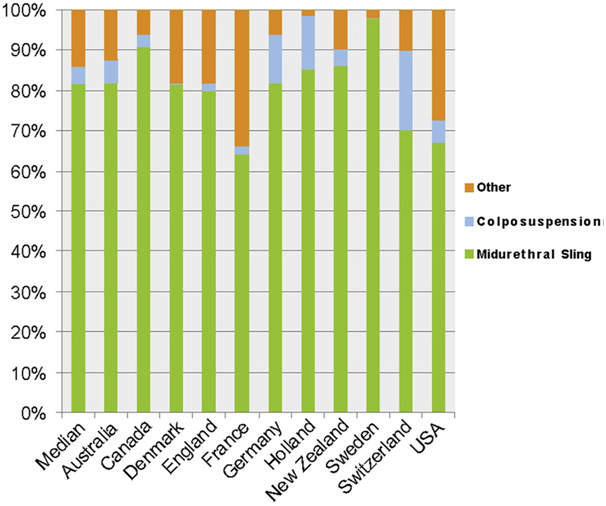
Midurethral sling procedures (MUS) are currently the most commonly performed operations for stress urinary incontinence (SUI), and have proved to be effective and safe. In Australia since its introduction in 1998, MUS have been the most frequently performed female continence surgery with over 80% of all SI operations. In a survey of 15 OECD counties in 2012 (Haya et al 2015) 82% of all SI operations were MUS. Other continence surgery includes fascial pubovaginal slings, Stamey needle suspensions, Botox injections, sacral nerve stimulators, and reconstructive bladder interventions that accounted for a median rate of 10.6% of continence interventions with considerable geographical variation that ranged from 1.3% in Holland to 34.3% in France.
MUS slings utilizing monofilament polypropylene mesh have the most favourable safety and efficacy results to date. Current data reflect concerns regarding the long-term efficacy of biological slings. Systematic reviews and meta-analyses of randomized controlled trials (RCTs) comparing a retropubic and a transobturator approach have demonstrated equivalence in early to midterm efficacy. The retropubic approach has a greater risk of bladder injury; the transobturator approach is associated with more vaginal perforations and groin pain, though fewer pelvic hematoma. For women with SUI and low closure pressure urethra, the transobturator route is less effective than the retropubic approach. Available RCT data are inadequate for definitive conclusions regarding the choice of slings in other important subgroups of patients, including those with recurrent incontinence, those undergoing concomitant prolapse surgery, the elderly, and the obese.
Recent global data suggests shows 47% of MUS preformed use the retropubic approach, 38% transobtrurator and 15% are single incision (SIS) MUS: This sling has an incision in the vagina only. Of the currently available “mini-slings” there is little comparative data and the RANZCOG would therefore recommend use of these types of slings only within the setting of a properly conducted clinical trial.
The choice of stress incontinence procedure is based on the surgeon’s experience as well as clinical grounds. The best results are often achieved with a procedure that works best in the individual surgeon’s hands.
References:
Ford AA, Rogerson L, Cody JD, Ogah J. Mid-urethral sling operations for stress urinary incontinence in women. Cochrane Database of Systematic Reviews 2015, Issue 7. Art. No.: CD006375. DOI: 10.1002/14651858.CD006375.pub3.